“Misty” is a 4-year old F/S English Setter presented to her veterinarian for inappetance and weight loss. She had lost 6 lbs in the course of 3-weeks. She had an occasional, rare dry cough, but no other specific clinical signs were reported. The working diagnosis based on a brief non-descript ultrasound exam, i.e., flash, targeted POCUS, by the referring veterinarian, untrained in AFAST®, TFAST® and Vet BLUE® formats, was a stump pyometra. Vet BLUE® stands for veterinary brief lung ultrasound exam (or in emergency) and “blue” also infers cyanosis.
When AFAST®, TFAST® and Vet BLUE® are combined into a single ultrasound examination we call the study Global FAST®. Moreover, we recommend Global FAST® for all patients providing an unbiased set of data imaging points that prevents imaging interpretation errors such as “satisfaction of search error” and “confirmation bias error” due to selective or targeted imaging, as well as allowing to determine if disease is localized or disseminated, and what other diagnostic sampling possibilities exist.
“Misty” presented to me for a complete abdominal ultrasound (AUS) (I am board certified in small animal internal medicine (ACVIM) and my mobile consulting practice includes advanced thoracic and abdominal ultrasound imaging since the 1990s and Global FAST® more recently since 2010). The AUS showed no specific abnormalities to explain her clinical signs and a stump pyometra was not present. Thoracic radiographs (TXR) were recommended for additional evaluation. The referring veterinarian was reluctant to perform TXR because it was felt that the cough was insignificant (dry, sporadic, and rare) based on the dog’s clinical profile and unremarkable lung auscultation. However, the referring veterinarian was persuaded to allow me to perform a Vet BLUE® examination. We call this the “baby step” to get to the TXR or CT.
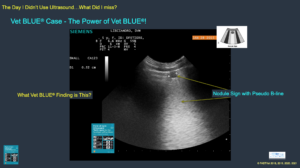
Fig. 1: Nodule Sign during Vet BLUE® (our created term now in our peer-review literature) due to fungal pneumonia. Nodules may also be seen with neoplasia and other non-fungal forms of granulomatous pneumonia as mentioned above including fungal, verminous (parasites), and bacterial. Note its size as 0.52 cm and having a pseudo B-line associated with it.
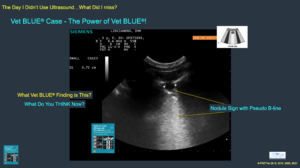
Fig. 2: Nodule Sign during Vet BLUE® at another view. Note the bright pseudo B-line extending from the deep surface of the nodule through the far field without fading. This sign can be seen in the adjacent images. The Nodule Sign requires a “pseudo B-line” (our created term now in our peer-reviewed literature, Pacholec et al. 2021). This one is 0.72 cm and note that there are 2 more smaller nodules with their pseudo B-lines stacked along the backside of the larger one.
Interestingly and importantly, the Vet BLUE® was low impact with minimal to no restraint, no shaving of hair, and performed in less than 2-minutes with real-time imaging information. There was no evidence of alveolar-interstitial edema. In other words, there was an absence of ultrasound lung rockets also called B-lines. However, multiple focal nodules were evident in the following lung regions: Left cranial lung lobe region- Nodule (5.2 mm), right caudal lung lobe region- Nodule (3.3 mm); right perihilar region- Nodule (7.2 mm); right middle lung region- Shred (6.5 mm). The findings suggested multifocal nodular disease and TXR was now indicated.
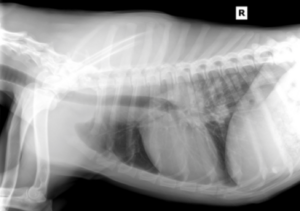

Fig. 3: TXR showing hilar lymphadenopathy and a suspicious patchy nodular interstitial pattern in the caudal lung fields.
Given the dog’s age and travel history, fungal disease was considered most likely; however, neoplasia could not be entirely ruled out. TXR was subsequently performed and showed hilar lymphadenopathy and patchy interstitial infiltrates especially in the left caudal lung lobe. Based on these findings, fungal titers were submitted and diagnostic for Coccidiomycosis. Itraconazole was started within 48-hours of my consult and the Vet BLUE®.
The take home message of this week’s blog is that Vet BLUE® is a rapid lung screening test that is far more sensitive than lung auscultation and chest radiography (well documented in the human literature). We have performed hundreds of Vet BLUE® examinations (created the format in 2010, and banked 400+ cases over the first 2-years, unpublished data) and have published several clinical research comparing Vet BLUE® findings with thoracic radiographs and CT.

Figure 4. These Nodules that are 0.52 and 0.72 cm (and others not shown) are completely occult, missed, along the lung surface on the radiographs. By using Vet BLUE® the nodules are found and the work-up more accurately pursued with the diagnosis made at the initial diagnosis. This is great care!
As an internist, I have found Vet BLUE® invaluable in my internal medicine practice, and in fact, in the past 2-weeks alone, I have had 4 cases with similar results. All 4 cases presented for abdominal ultrasound but lung pathology was detected using the addition of Vet BLUE® and that were subsequently confirmed with TXR.
The fundamental Vet BLUE® 6 lung ultrasound findings are easily teachable and include: Dry lung (lung sliding and A-lines), wet lung (ultrasound lung rockets also called B-lines), Shred Sign, Tissue Sign, Nodule Sign, and Wedge Sign (our created term). Using the Vet BLUE® pattern-based approach, more evidence-based lung information is provided over routine means of lung auscultation and thoracic radiography (TXR). An excellent diagnostic algorithm for lung ultrasound findings is in the textbook Point-of-care Ultrasound Techniques for the Small Animal Practitioner, 2nd Edition, Wiley ©2021
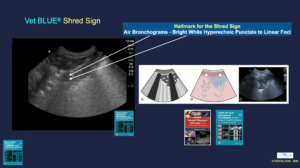
Figure 5. Shred Sign
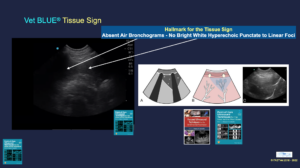
Figure 6. Tissue Sign
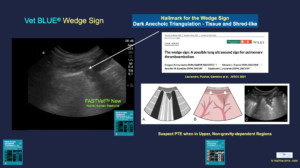
Figure 7 Wedge Sign
Assumptions are made in using Vet BLUE® and that acute conditions including neoplastic and granulomatous lesions make it to the lung periphery. This is an important potential limitation of Vet BLUE® since that unless the disease or condition makes it to the very outer surface of lung at one of its acoustic windows, the pathology goes undetected ultrasonographically. Therefore, Vet BLUE® cannot replace TXR and should be used in conjunction with TXR. However, it has been shown in human medicine that most acute conditions do in fact make it to the lung periphery, and lung ultrasound is an effective means of diagnosing and recognizing lung pathology otherwise missed by lung auscultation and routine chest radiography in people. Moreover, you will quickly see how nebulous pathology on TXR, or no surface pathology on TXR, is clearly evident using Vet BLUE®. In this case, note the various sizes of the nodules at various Vet BLUE® regions that were occult on TXR.
The bottom line in this case (just think about the possibilities ) is that this patient would have been sent home without the correct diagnosis (or its suspicion) and with a course of ineffective antibiotics. It is possible (and likely) that the dog may not have returned until the disease was significantly more advanced and “Misty” was showing more significant respiratory signs including respiratory distress. The outcome may not have been successful as a result of such a possible and likely delay plus its inaccurate treatment.
The use of Vet BLUE® has been invaluable in my internal medicine practice. In this case, Vet BLUE® helped me “capture” the case early in its course, when treatment would be more effective, rather than waiting until the patient presented with advanced disease, i.e., snowstorm lungs, and in respiratory distress. As we say “FAST (and Vet BLUE®) Saves Lives!”
FASTVet Premium members have access to all of our archived blogs and our video library. Take our Online Vet BLUE®-Global FAST® Course – 7-hours – that is RACE-approved for greater detail.
Side Notes – this patient could be monitored using Vet BLUE®
Vet BLUE® B-line Scoring System

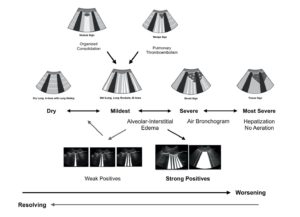
Vet BLUE® Visual Lung Language

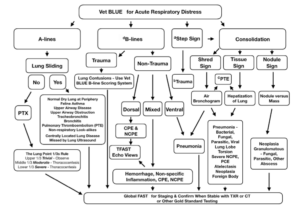
Vet BLUE® Algorithm (see others in our 2nd edition textbook)
Send any comments to Dr. Greg Lisciandro, DVM, DABVP, DACVECC at LearnGlobalFast@gmail.com
gl/GL 4-9-2024