The “Asynchronous Curtain Sign (ACS)” has been described as a finding in patients with pneumothorax (PTX). In my opinion, the ACS is the same as a previous clinical study in dogs that described the phenomenon as “Reverse A-lines.” The location for the finding is the “highest” region at the transition zone of pleural and abdominal cavities, originally referred to as the TFAST® Chest Tube Site view, where free air in the pleural space would rise to in the presence of PTX.
The transition zone, anywhere along the interface of pleural cavity and abdominal cavity, and described with Vet BLUE® at its Caudodorsal, Perihilar, and Middle Lung Regions, have this “curtain effect” where air in the pleural cavity will cover and uncover with a linear border the abdominal structures in synchrony with phases of respiration. This has been described as the “Curtain Sign of Lung Ultrasound”, with a similar phenomenon as the better known “Curtain Sign of Pleural Effusion.”
To reiterate, in normal the pleural side and abdominal side of this interface move in synchrony with phases of respiration. With inspiration and expiration each side of the interface, transition zone, move together. In PTX it has been described by Hwang et al, and Boysen et al. that the pleural side and abdominal side move asynchronously moving toward one another and then away from one another with phases of respiration called “Reverse A-lines” and “Asynchronous Curtain Sign”, respectively.
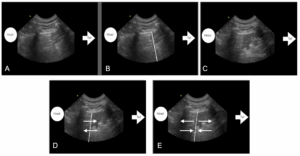
Figure by Lisciandro GR showing the “Curtain Sign of Lung Ultrasound” with the air shadowing to the left, and abdomen to the right with the linear border unlabeled in A) whereas the same image in B) has an overlay for the linear “curtain-like” border that in real-time would cover and uncover the abdominal structures in synchrony with phases of respiration; when compared to C) the image would be in inspiration. In C) the patient has expired (in expiration) and the liver in the near field could be mistaken for lung consolidation called the “Tissue Sign”, the rugal folds mid screen mistaken for lung consolidation called the “Shred Sign”, and far field the gastric contents with “Pseudo gastric B-lines” that can be mistaken for “wet lung” and types of alveolar-interstitial edema (Lisciandro’s mantra of “blood, water, or pus”). For the reasons it is important that the “Curtain Sign of Lung Ultrasound” be recognized and then lung imaging cranial to this transition zone of pleural and abdominal cavities. In D) the pleural and abdominal sides move in synchrony with phases of respiration as indicated with the arrows. In E) the pleural and abdominal sides are moving away from each other and then toward each other in asynchrony which is unexpected in normalcy and may be associated with PTX however other respiratory conditions that results in paradoxical abdominal breathing can create the asynchrony as well in the absence of PTX.
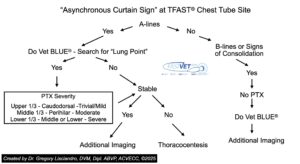
This is important for veterinary professionals using point-of-care ultrasound to be aware at triage since the finding of the “Asynchronous Curtain Sign” is not pathognomonic for PTX. Moreover, PTX is a “dry artifact” phenomenon, and thus A-lines would be present within the “Curtain Sign” without any “wet lung” artifacts, i.e., B-lines also called “lung rockets”, or any other findings of lung opposed to the thoracic wall during imaging, i.e., Vet BLUE® signs of consolidation called Shred, Tissue, Nodule, and Wedge Signs. A Clinical Algorithm has been created by Lisciandro GR.
Here is a short video showing examples of synchronous and asynchronous curtain signs with case examples. THIS VIDEO WILL PLAY but has a SHORT SEVERAL SECOND DELAY and lasts in total about 90 seconds. Enjoy the didactic video short. THERE is NO SOUND.
grl/GLR 7-28-2025