ECC and IM Blog – Must Read and Watch – Nonspecialist Practitioner (NSP) Screening Echo Views for Cats
This Loughran et al. is an interesting feline study evaluating echo views as a 2-minute screening test for feline heart disease by nonspecialist practitioners (NSP) and the focus of this ECC and IM Blog.
They refer to this test as “an extension of the feline physical exam” in the You Tube Instructional by Dr. John Rush, DVM, DACVIM (Cardiology) – see LINK below.
The study was published in the Sept-Oct 2019 issue of the Journal of Veterinary Internal Medicine (JVIM) and is “Open Access” thus you can obtain the text in full:
The study’s 2-minute echo approach emphasizes similar TFAST views that Global FAST Course alumni have been trained to do:
1) The Left atrial to Aortic Ratio (LA:Ao) on short-axis from the right side (parasternal/pericardial view)
2) The Left Ventricular Short-axis “Mushroom view” (LVSA) from the right side (parasternal/pericardial view)
Here is a nice didactic Echo Instructional for Cats by Dr. John Rush, DVM, DACVIM (Cardiology) from Tufts linked to the Loughran et al. JVIM Study
Criteria for Capturing Abnormal Cats Using their 2-minute Echo Screening Test
A) Hypertrophic Cardiomyopathy (HCM) Cats – Most Common Type of Feline Heart Disease
1) The left atrium is considered “enlarged” by the following findings:
A short-axis (SAX) left atrial diameter > 1.5 the aorta (LA:Ao > 1.5) – we refer to as the “Traditional Linear Method” A short-axis (SAX) left atrial area that could fit > 2.5-3 aortas – we refer to as the “John Rush Area Method”
NOTE: the Eyeball Method is much less reliable in cats – Freeze and Roll the Cine Ball through frames
2) The left ventricular wall is considered “thick” by the following findings:
The left ventricular on SAX being > 40% the left ventricular cavity diameter
The left ventricular papillary muscles on SAX subjectively appearing prominent
The left ventricular filling on SAX subjectively being small in systole
NOTE: the Eyeball Method is much less reliable in cats – Freeze and Roll the Cine Ball through frames
B) *Dilated Cardiomyopathy (DCM) Cats
1) Poor left ventricular contractility by the following:
If the left ventricle does not contract more than 50% on SAX during systole
If the vigor of the left ventricular contractions on SAX appear subjectively less than normal
*Dilated Cardiomyopathy is rare in cats
C) #Pleural Effusion (PE) and Pericardial Effusion(PCE)
1) Teaching for the NSP was based on video clips – so in other words “it looks like PE or PCE”…a better approach…
2) The FASTVet rules for the accurate TFAST diagnosis of PE and PCE include the following and avoid the sonographer mistaking heart chambers for PE or PCE or both:
Always image the heart in its entirety using the bright (hyperechoic) pericardium as a landmark in the far field
Image toward the muscular apex of the heart where it is unlikely to mistake a heart chamber for PE or PCE
Racetrack Sign via the FAST Diaphragmatico-Hepatic (DH) View
Bull’s Eye Sign via the right TFAST Pericardial Site view
The Long-axis 4-chamber View in which all 4 chambers may be identified and thus effusion clearly outside of the heart
NEVER diagnose solely on the Left Ventricular Short-axis (SAX) Views as it is too easy to mistake the crescent shaped right ventricle for PE or PCE
Saving cine clips (video clips) is helpful so that they may be reviewed after placing the cat in oxygen. This allows further review without the stress of image acquisition and the patient.
#Pericardial Effusion is important because the most common cause in cats (>75%) is congestive heart failure, a treatable disease (Hall et al. JVIM 2007; Ward et al. JVIM 2018)
Some FASTVet notes from the JVIM Study article:
Abbreviations:
Ao: aorta
FCU: Focused Cardiac Ultrasound
JVIM: Journal of Veterinary Internal Medicine
LA: left atrium
LAX: long-axis
LVSA: left ventricular short-axis view
NSP: Non-Specialist Practitioner
PCE: pericardial effusion
PE: pleural effusion
POC: point-of-care
POCUS: point-of-care ultrasound
SAX: short-axis
TFAST: thoracic FAST
Numbers of Cats Enrolled:
1) 343 cats, none sedated, 28 removed because fractious, 26 cats because of inadequate image acquisition (84% success rate)
2) Each NSP contributed a median number of 11 cases
3) Median cat age 9-years
4) Median cat weight 5.2 kilograms
5) Cats – 114 females, 175 males
6) Heart rate and respiratory rate were not helpful
7) Use of Physical Exam (murmur, gallop), ECG was also not helpful to screen cats
8) Most effective was the addition of Focused cardiac Ultrasound (FCU)
9) Interestingly, the addition of POC-BNP did not add any additional diagnostic value over the FCU in this study
Section 1
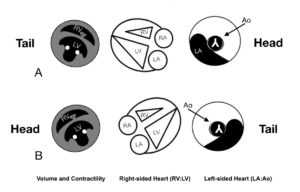
1) The cardiologist’s images are mirrored from the manner we teach. The cardiologist reverses the screen orientation with the head to the right and tail to the left. We keep ALL imaging the same no matter the region on the patient with the head to left of the screen and the tail to right. The head to the left orientation is standard for AFAST, TFAST and Vet BLUE and for lateral radiography. When viewing a cardiologist’s echo views you will have make mental adjustments. Here are the TFAST echo views in charts with an overlying Clock Face – see Section 3 – in the Classic Cardiologist Orientation and the Rogue Global FAST Orientation…
Again, the cardiologist reverses the screen orientation. The positioning and centering of the image is thus backwards from saying placing the kidney or urinary bladder in the center of the screen. In other words we do not reverse the orientation but keep the same orientation for all Global FAST imaging no matter what is being imaged. If you have learned the our TFAST echo methodology and you want the cardiologist orientation, you have 2 choices – 1) you can rotate the probe marker 180 degrees while still using the 4 o’clock short-axis (SAX) line or 2) use the “reverse button” feature. See Section 3
Of note: In human point-of-care ultrasound (POCUS) training, many institutions do the same as we teach and do NOT reverse the orientation marker during echo views seeing the importance of keeping all ultrasound imaging consistent.
Cardiologists who are now understanding the importance of the Global FAST Approach are facing similar orientation challenges because of the historical reversal of the marker for echo views. Some of the veterinary cardiologists we know are now scanning lung (Vet BLUE) and abdomen (AFAST) with the same consistent orientation as their echo views because of the spatial problems created when “reversing” from cardiac to lung and abdomen.
Section 2
2) Assessment for increased left atrial (LA) size by the “Traditional Linear Method” and the “John Rush Area Method.” We like his approach as well because it’s a good way to double check yourself by comparing both the “Traditional Linear Method” and the “John Rush Area Method” to one another.
The comparison of the 2 methods for estimating left atrial enlargement
in a normal LA:Ao cat. Copyright 2019 Greg Lisciandro, DVM, FASTVet.com
The comparison of the 2 methods for estimating left atrial enlargement
in an abnormal LA:Ao cat. Copyright 2019 Greg Lisciandro, DVM, FASTVet.com
We like both the “John Rush Area Method’ and the “Traditional Linear Method.” By using both methods, it’s a good way to double check yourself.
Section 3
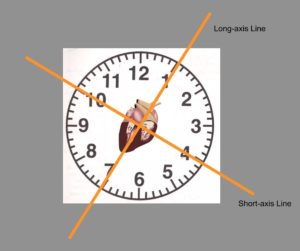
3) The probe marker is directed to ~ 4 o’clock and then fanned while staying on the 4 o’clock short-axis line through the various short-axis (SAX) views – see Section 1. The common mistake is rotating your hand off this SAX line while fanning – most often by erroneously rotating to 3 o’clock. The key here is to constantly check your probe to make sure you are on the 4 o’clock SAX line and if not, self correct.
Note the manner in which a cardiologist does the view, the probe marker would be on a 10 o’clock line (180 degree reversal). Some machines have an automatic “reverse” button that will change the screen for you without you having to rotate your probe. Look for this feature on your machine:
The “Reverse” button on the keyboard of a GE Logiq e
Find these buttons on your Keyboard and place those colored adhesive or sticker dots next to these buttons. The way to easily tell how they change the image is to place the probe on YOUR soft tissue neck area with beating vessels (carotids) and play with these knobs! And do the same on your patients spleen and urinary bladder.
We have found the FASTVet “Clock Face Approach” modified from Oncura Partners to be very effective for teaching short- and long-axis echo views. See Section 1
Section 4
4) The Focused Cardiac Ultrasound (FCU) study describes pleural effusion (PE) and pericardial effusion (PCE) yet gives no information on these results, the presence and absence of either. A JVIM reviewer should have caught the oversight.
FASTVet teaches from data shown in feline clinical studies, that the presence of PE and PCE, in addition to echo views, is clinically impactful for the patient’s working diagnosis. The presence of PCE places congestive heart failure, a treatable disease, at the top of the working diagnosis (Hall et al. JVIM 2007; Ward et al. JVIM 2018) and argues against the “flash” approach.
Section 5
5) No discussion is mentioned regarding what we refer to as the Global FAST Fallback Views, another FASTVet original concept . These Global FAST Fallback Views are important because they are often easier and less risky for the feline patient (and canine and other species) over echo views. The premise is that absent B-lines all Vet BLUE views effectively rules out left-sided congestive heart failure (Lisciandro et al. JVECC 2016; Ward et al. JAVMA 2017); and a bounce (height changes of 35-50% during respiratory and cardiac cycles) to the caudal vena cava without hepatic venous distension as the caudal vena cava crosses the diaphragm at the FAST Diaphragmatic-Hepatic (DH) View rules out right-sided congestive heart failure.
Thus, when the feline patient has equivocal echo views the Global FAST Non-echo Fallback Views provide additional clinically relevant information; and when the echo views are unattainable, the Global FAST Fallback Views can help dictate how urgently a complete echo study is needed.
The use of the Global FAST Non-Echo Fallback Views in patients
with left atrial and right ventricular enlargement.
Modified from Focused Ultrasound Techniques for the Small Animal Practitioner, Wiley Copyright 2014 and Greg Lisciandro, DVM, FASTVet.com Copyright 2019
Section 6
6) The “S probe” stands for “Sector probe” which is the same as a “Phased-array” probe and are advantageous for cardiac imaging because their small focal point optimizes imaging of the heart by eliminating rib shadows. Probe and transducer are synonymous. In the You Tube Instructional Video the something like S12-4 and the S8-3 and the S5-1 probes are mentioned. The numbers after the letter indicate the frequency range so “S12-4” has a range of 12MHz to 4MHz and the “S8-3” has a range of 8MHz to 3MHz and so forth. The same letter and number system holds true for convex and linear probes.
Screen Shot from the You Tube Video by Dr. John Rush
Most of you will have microconvex probes with a frequency range of 5-10 MHz which will be fine for imaging cat hearts with the disadvantage of rib shadows. A linear probe distorts the heart too much, generally does not provide adequate depth as well, plus other inherent factors.
Section 7
7) Lastly a repeat evaluation 2-4 weeks later and then every few months would have been a good recommendation by this study in questionable cats THAT is not mentioned. Repeating the exam is always a good rule of thumb in my book : ) and eliminates the pressure of an equivocal study along with integrating the Global FAST Approach and its Fallback Views for evidence of congestive heart failure.
Always do a Global FAST!
Buy our Big Saving Bundle
We are BUNDLING the AFAST®-TFAST®-Vet BLUE®-Global FAST® Online Course Fee for a signup of ALL 3 Courses for $895.